Acid Reflux and Hiatal Hernia
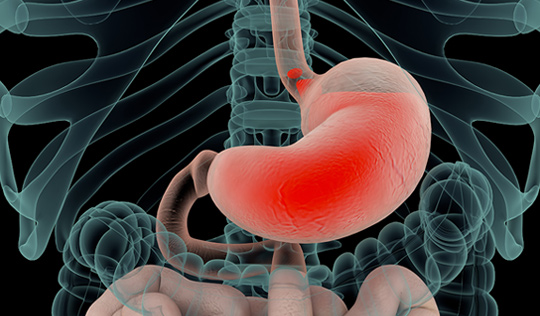
Gastroesophageal reflux disease (GERD), commonly known as acid reflux, is one of the most common gastrointestinal disorders. It refers to abnormal reflux of stomach acid and food into esophagus, causing heartburn, regurgitation, sore throat, chronic cough, change in voice and aspiration pneumonitis. Rarely, patients may develop pre-cancerous changes in lining of esophagus referred to as Barrett’s esophagus. GERD may occur as a result of weakening of the lower esophageal sphincter muscle. GERD may also be due to a hiatal hernia.
Hiatal hernia occurs when the upper part of the stomach slides up into the chest through an opening in the diaphragm, called the diaphragmatic hiatus (diaphragm is a dome-shaped muscle separating the abdomen from the chest). Hiatal hernia results in abnormal functioning of the lower esophageal sphincter. Hiatal hernias are very common, and their exact cause is not well understood. They may be hereditary. They are often associated with spinal deformities such as kyphosis or scoliosis. They are also seen frequently in individuals with excess weight.
Very often, patients may have no symptoms and their hernia may have been found incidentally during routine X-rays. In others it may cause symptoms of acid reflux, abdominal pain, chest discomfort, bloating, and difficulty with swallowing. Occasionally patients experience complications such as volvulus and strangulation of the stomach (when the stomach gets twisted in a way that cuts off blood supply). Rarely hiatal hernias present with atypical symptoms such as recurrent pneumonia, chronic cough, hoarseness of voice, or anemia of unknown etiology.
Hiatal hernia and its para-esophageal variant require surgical treatment if they cause moderate to severe symptoms, or if the stomach is at danger of volvulus and strangulation. GERD in absence of hiatal hernia may also require surgery in order to improve quality of life. This is often seen in patients with GERD whose symptoms are not controlled with acid suppressive therapy, or in those concerned about side effects of long-term medication usage. In addition, surgery is helpful to prevent progression of Barrett’s esophagus – a pre-cancerous condition in the lining of lower esophagus caused by chronic exposure to acid.


Robotic-assisted laparoscopic surgery has revolutionized surgical treatment of hiatal hernias. Robotic instruments mimic the wristed motion of a surgeon’s hand, robotic optics offer magnified high definition view of structures in 3-D, and because incisions are 8 mm in size, there is minimal pain after surgery.
During surgery, which is performed under general anesthesia, Dr. Zaré makes 5 small incisions in the upper abdomen. Using the robotic platform, stomach and lower esophagus are reduced back into the abdominal cavity from the chest.
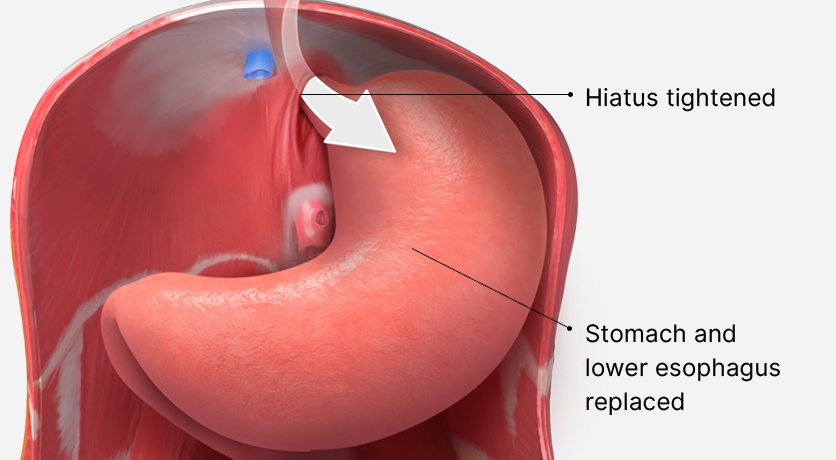
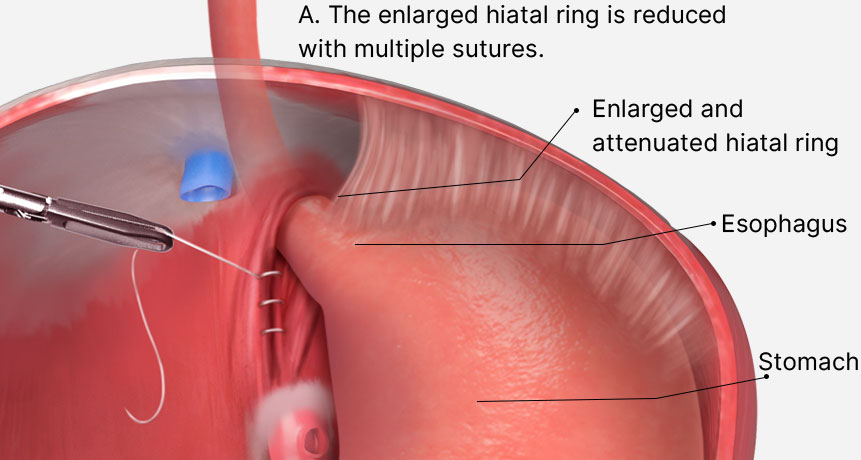
The hiatal hernia, which is formed by enlargement of the diaphragmatic crura, is then repaired with multiple permanent sutures. To prevent recurrence of the hernia, a biologic dermal matrix is sutured to the diaphragmatic crura.
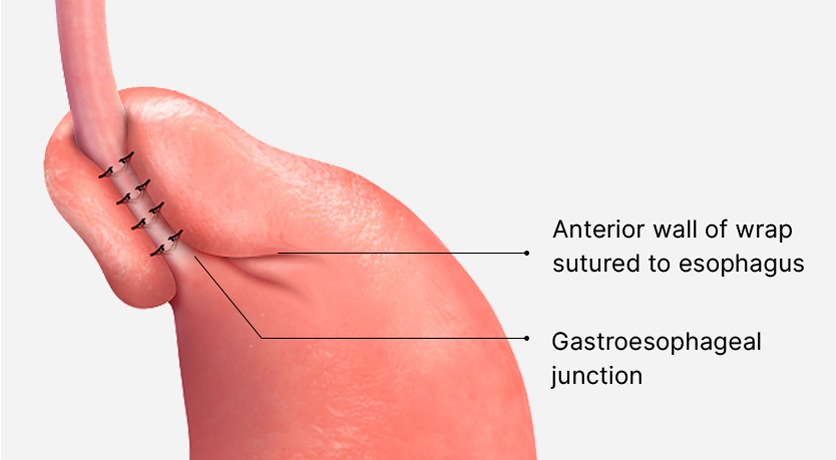
Next, a fundoplication or wrap is created to prevent acid reflux. There are many types of fundoplication. Dr. Zaré favors the Toupet fundoplication, also referred to as posterior partial 270-degree fundoplication. To create a Toupet fundoplication, the esophagus and the fundus of the stomach are dissected free the surrounding tissue. Part of the fundus is then brought through a window behind the esophagus and sutured to the opposing side.
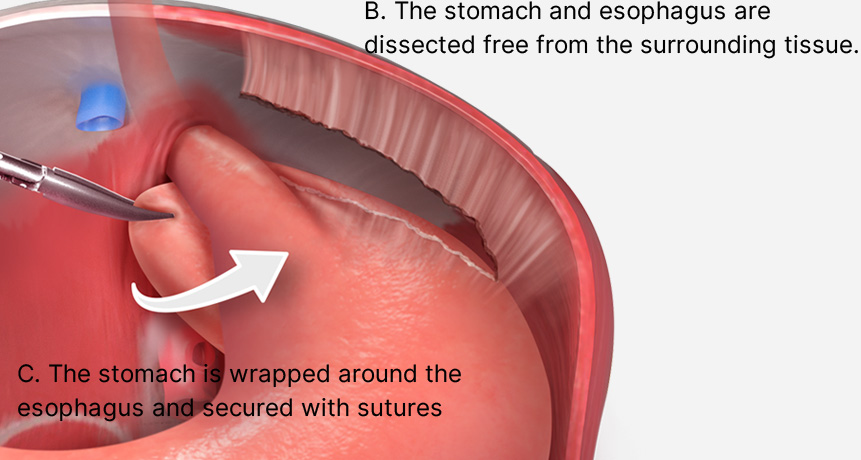
The Toupet fundoplication has the appearance of a ‘bun and a hot dog’. Because the fundoplication covers three quarters of the esophageal circumference, it is gentler than Nissen fundoplication which covers the entire circumference. Toupet fundoplication is associated with a lower incidence of bloating after surgery.
After surgery, patients spend one night in the hospital, return to day to day activities within 2-3 days, and resume unlimited activities within 2-3 weeks. Majority of patients are able to stop their acid suppressive therapy and resume a normal lifestyle.
